arXiv: 2604.20022 · PDF
作者: Yusuf Kesmen, Fay Elhassan, Jiayi Ma, Julien Stalhandske, David Sasu, Alexandra Kulinkina, Akhil Arora, Lars Klein, Mary-Anne Hartley
主分类: cs.LG · 全部: cs.AI, cs.CL, cs.LG
命中关键词: large language model, llm, agent, rag, reasoning, inference
TL;DR
BMBE 把 LLM 降级为"传感器",把医疗诊断推理交给可审计的贝叶斯引擎,模块化架构在精度、隐私和鲁棒性上超过独立 frontier LLM。
核心观点
- LLM 把"自然语言沟通"与"概率推理"混在一起是架构缺陷,而非工程瑕疵。
- 应严格分离语言层与推理层:LLM 只做解析和措辞,贝叶斯引擎承担全部诊断推断。
- 由于患者数据不进入 LLM,架构天然私密;统计后端可按人群替换,无需重训。
- 带来三大独有特性:可调的 selective diagnosis 精度-覆盖权衡、“统计分离 gap”,以及对抗性患者语气下的鲁棒性。
方法
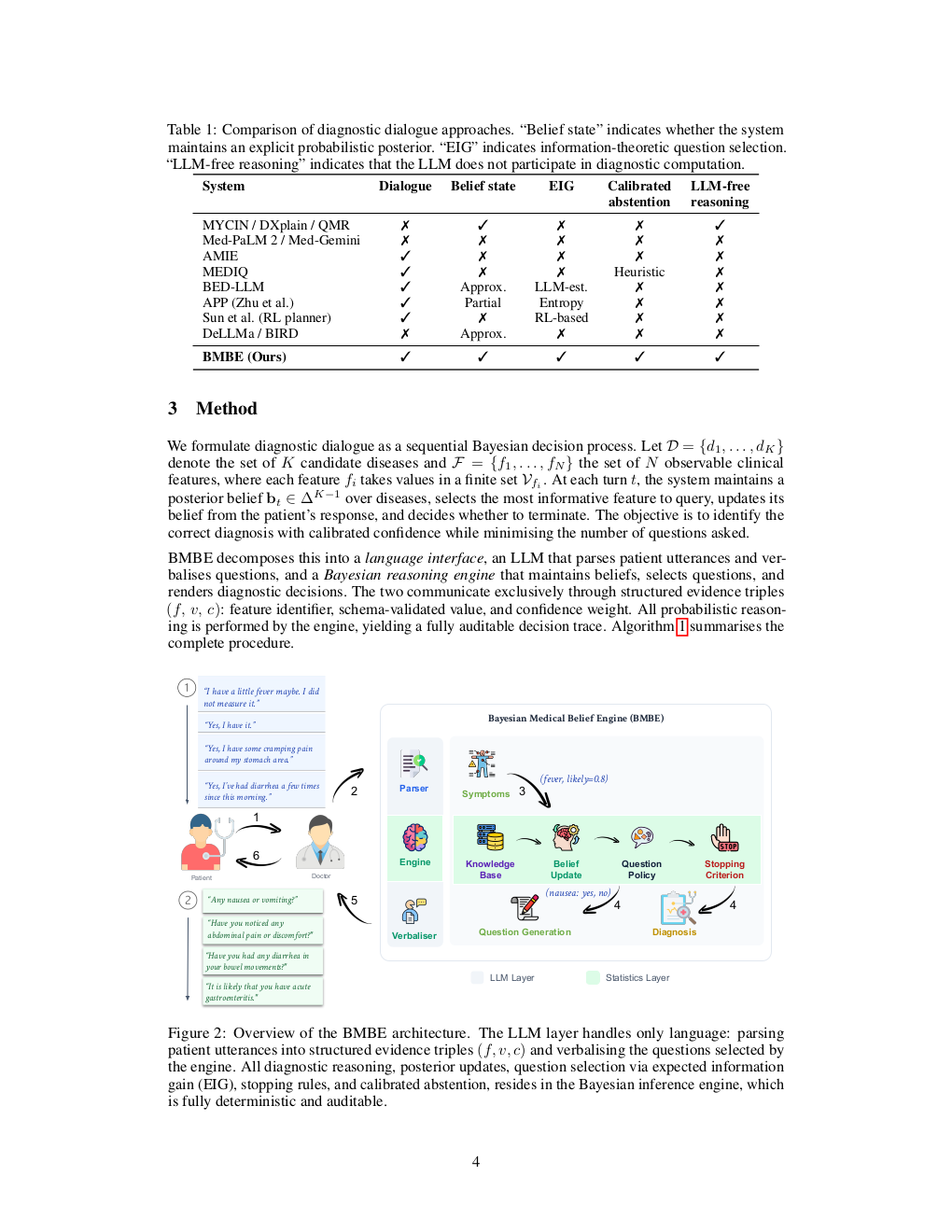
提出 BMBE (Bayesian Medical Belief Engine),模块化对话诊断框架:
- LLM as sensor:解析患者自由文本为结构化证据,并把引擎要问的问题口语化。
- Bayesian engine:确定性、可审计的概率推理核心,基于知识库维护疾病后验,决定下一步询问和何时给出诊断。
- Selective diagnosis:通过阈值连续调节 accuracy–coverage 折中。
- 统计后端可独立替换以适配不同人群。
实验
- 在经验知识库与 LLM 生成知识库两类设置上评测。
- 基线为同家族的 frontier standalone LLM(autonomous diagnostic agent)。
- 指标覆盖诊断准确率、覆盖率、成本,以及对抗性沟通风格下的稳健性。具体数据集名称摘要未披露。
结果
- 廉价 sensor + 贝叶斯引擎可超越同家族 frontier 独立模型,成本只是后者一小部分,呈现"统计分离 gap"。
- 可连续调节精度-覆盖曲线,独立 LLM 无此能力。
- 在对抗性患者语气下,独立模型性能崩溃,BMBE 保持稳健。
- 具体数值摘要未给出,需看正文。
为什么重要
对医疗 agent、隐私合规系统和 LLM infra 从业者:展示了一条"不靠 scale、靠架构"的路线——把不确定性推理从 LLM 里抽出来交给可验证模块,可同时拿到隐私、可审计性、成本优势和可控的弃答机制,对高风险领域部署有直接借鉴意义。
与已有工作的关系
- 延续 LLM-as-diagnostic-agent 方向(如 AMIE、Med-PaLM 式对话诊断)。
- 呼应 neuro-symbolic 与 tool-augmented LLM 思路,把确定性推理外置。
- 贝叶斯引擎部分承袭经典 medical expert system / Bayesian network 诊断(QMR-DT 等)。
- selective prediction / conformal 风格的 accuracy-coverage 折中亦有先例。
尚未回答的问题
- 在真实临床数据和多语种、多文化人群上的外部效度?
- 知识库构建与维护成本,尤其贝叶斯网络结构与条件概率的获取与更新?
- 解析式 LLM sensor 的错误如何传播进后验,是否需要不确定性估计?
- 面向多轮长程病史、多病共存、检验结果整合的扩展性?
- 与临床工作流、医生监督的交互形态与监管合规路径。
论文图表
图 1: Page 2 (rendered)
图 2: Page 3 (rendered)
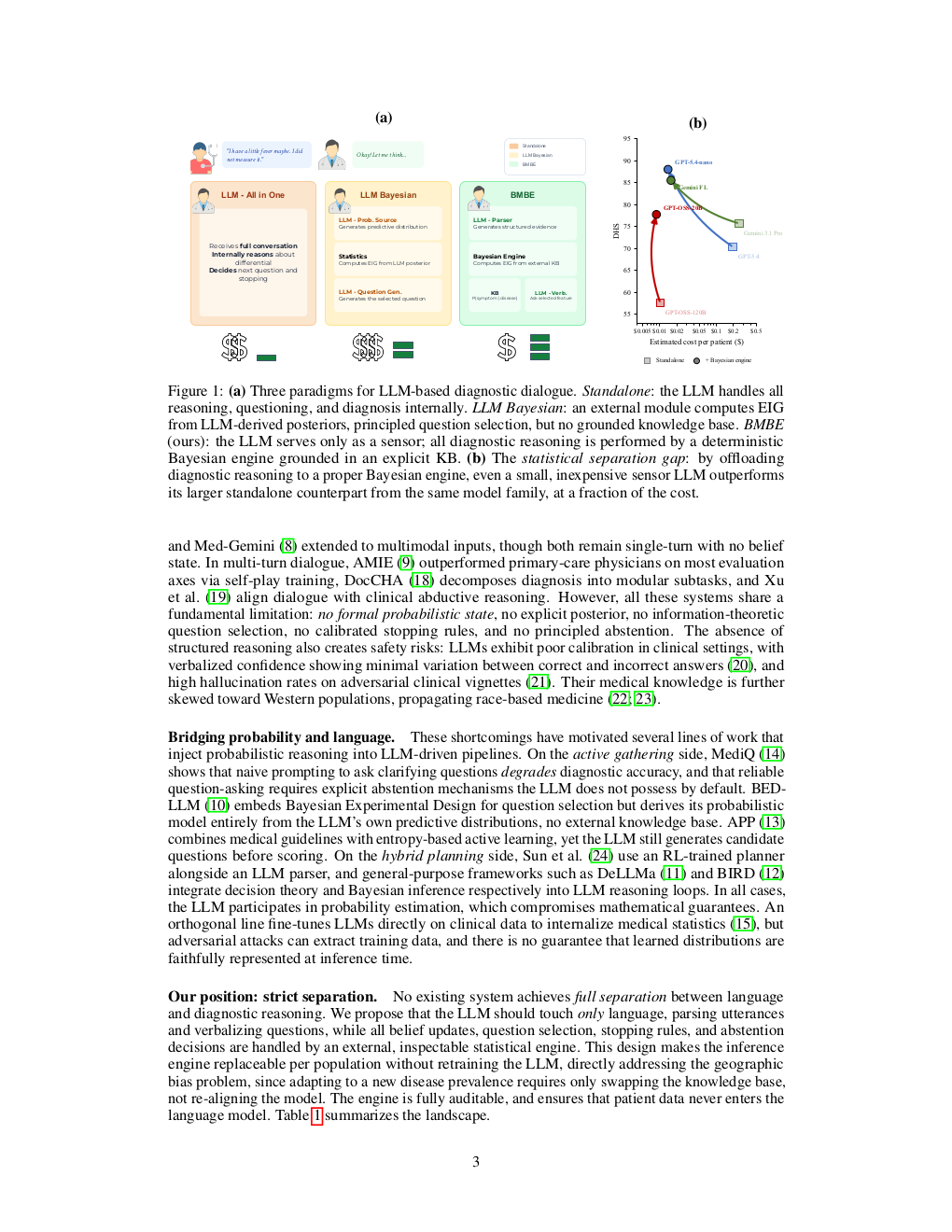
图 3: Page 4 (rendered)
原始摘要
Large language models are increasingly deployed as autonomous diagnostic agents, yet they conflate two fundamentally different capabilities: natural-language communication and probabilistic reasoning. We argue that this conflation is an architectural flaw, not an engineering shortcoming. We introduce BMBE (Bayesian Medical Belief Engine), a modular diagnostic dialogue framework that enforces a strict separation between language and reasoning: an LLM serves only as a sensor, parsing patient utterances into structured evidence and verbalising questions, while all diagnostic inference resides in a deterministic, auditable Bayesian engine. Because patient data never enters the LLM, the architecture is private by construction; because the statistical backend is a standalone module, it can be replaced per target population without retraining. This separation yields three properties no autonomous LLM can offer: calibrated selective diagnosis with a continuously adjustable accuracy-coverage tradeoff, a statistical separation gap where even a cheap sensor paired with the engine outperforms a frontier standalone model from the same family at a fraction of the cost, and robustness to adversarial patient communication styles that cause standalone doctors to collapse. We validate across empirical and LLM-generated knowledge bases against frontier LLMs, confirming the advantage is architectural, not informational.